Druggable proteins influencing cardiac structure and function ...

Popliteal Artery Entrapment Syndrome: An Approach To Diagnosis And Management
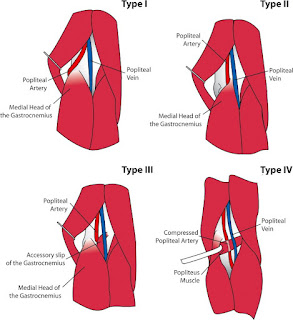
What is popliteal artery entrapment syndrome?Popliteal artery entrapment syndrome (PAES) is an anomaly resulting in symptomatic extrinsic compression of the popliteal artery by the surrounding musculotendinous structures; most frequently the medial head of the gastrocnemius muscle. This may be congenital or acquired through muscular hypertrophy. PAES can be further classified by anatomical type (I–VI, table 1). It may exist alone or in combination with popliteal vein and/or tibial nerve compression as part of popliteal entrapment syndrome.
View this table:Popliteal entrapment syndrome classification (Popliteal Vascular Entrapment Forum)6
PAES is a frequent cause of intermittent claudication in an otherwise healthy, often athletic cohort, with potentially severe adverse sequelae and can represent a diagnostic challenge.
CaseA 38-year-old female competitive 'ironman triathlete' athlete with no medical history presented with exertional left calf pain. On examination, the patient had a full complement of lower-limb pulses.
A lower-limb arterial duplex scan detected bilateral popliteal artery occlusion on forced plantar flexion. As there were unilateral symptoms, a CT angiogram was performed which detected no abnormality. A bilateral lower-limb angiogram initially demonstrated normal arterial anatomy. However, on forced plantar flexion, complete occlusion of both popliteal arteries was evident (figure 1).
Figure 1Lower-limb arterial angiogram at rest (left) and during forced plantar flexion demonstrating bilateral popliteal artery occlusion (right).
The patient was diagnosed with bilateral PAES and underwent staged popliteal artery releases. At 1 year …
Overview Of Exercise Induced Lower Leg Pain
Lecture 8
This paper discusses the common causes of exercise induced lower leg pain, including chronic compartment syndrome (CCS), medial tibial stress syndrome (MTSS) and chronic calf tears (CCT).
The pathogenesis, clinical presentation, diagnosis and treatment of the more popular conditions are discussed.
CCSs are due to an increased pressure in one or more of the four compartments of the lower leg, brought on by exercise and relieved by rest. Clinical examination of the limb is normal. Diagnosis is made by measuring the compartment pressures during exercise. Treatment is by a subcutaneous fasciotomy of the affected compartments.
MTSS is thought to be due to abnormal biomechanics leading to a periostalgia of the inner tibial border both during and after exercise, with symptoms lasting up to 24–48 h postexercise. Patients always locate their pain to the inner tibial border. Examination of the limb shows the lower and often the middle inner tibial border to be tender. Diagnosis is largely clinical but may be helped by MRI scans. Treatment is initially by physiotherapy in the form of flexibility and strengthening exercises and the fitting of orthotics. If this fails then major surgery is the only other alternative.
CCT occur as a result of scar tissue in the muscle or adhesions developing between the fascia and the muscle causing pain in the posterior aspect of the calf. Often there is a past history of an acute calf tear. The pain presents during a run and often the athlete will describe pain in the posterior aspect of the calf which will increase with the intensity of exercise and if they try to run through the pain they experience a tearing sensation in the calf muscle sufficient to stop them exercising and cause them to limp up to a period of 3 days. Clinical examination often reveals tenderness over the medial head of gastrocnemius. An MRI scan may or may not aide in the diagnosis. Treatment initially is in the form of physiotherapy and if this fails then operative surgery which carries an 80% success rate.
Finally other rarer causes of exercise induced leg pain are discussed, namely muscle hernia, popliteal artery entrapment syndrome, nerve entrapments and metabolic disorders.
Adventitial Degeneration Of The Popliteal Artery As A Rare Etiology Of Impaired Arterial Circulation In The Lower Extremities
A 30-year-old female patient presented to the emergency department with a 3-day history of intermittently impaired sensory function and sensation of cold in the right foot. The lower extremities both exhibited the same coloring, were both warm, and exhibited no motor deficits. The lower leg as well as the lateral and dorsal foot were hypesthetic on the right lateral side. Duplex ultrasound showed a monophasic signal in the vessels of the lower leg and prompted suspicion of a popliteal artery aneurysm with risk of vascular occlusion. From a differential diagnostic perspective, peripheral arterial occlusive disease was considered, although the patient's young age was untypical. Magnetic resonance imaging (MRI) with contrast-enhanced angiography was performed. This showed oval cystic structures associated with the popliteal artery and measuring up to 12 mm in diameter with consequent compression. This was caused by cystic adventitial degeneration. This rare disease primarily affects male patients (5:1) and is causal in 1/1200 cases of intermittent claudication. Surgical management revealed communication between the cysts and the joint space as well as inflammatory changes in the vessel wall over a 5-cm segment. This segment was removed and a vein interposition graft placed.
Figure
Magnetic resonance imaging (MRI)
Jakob Leonhardi, Samer Aldmour, Dr. Med. Jeanette Henkelmann, Klinik und Poliklinik für Radiologie, Universitätsklinikum Leipzig, jakob.Leonhardi@gmx.De
Conflict of interest statement: The authors declare that no conflict of interest exists.
Translated from the original German by Christine Rye.
Cite this as: Leonhardi J, Aldmour S, Henkelmann J: Adventitial degeneration of the popliteal artery as a rare etiology of impaired arterial circulation in the lower extremities. Dtsch Arztebl Int 2023; 120: 179. DOI: 10.3238/arztebl.M2022.0369



Comments
Post a Comment